
Ianis Stancof (L6R)
Antibiotics really formed one of the first bases of treatment that doctors of the time had to deal with growing infections. Antibiotics are credited with increasing the average life expectancy by 23 years ever since the circulation of penicillin in 1928 largely because infections which before could have even been fatal for some healthy patients could now be dealt with.
Whilst the drastic development from magic bullets like salvarsan 606 to eventually penicillin and now to over 100 antibiotics was a considerable milestone and a irrefutable tool that doctors have nowadays for treating a patient there has been steady decline in the effectiveness of antibiotics through the growing bacterial resistance that certain strains have developed as a result of numerous factors all of which is causing an increasing worry that antibiotics will become ineffective without stricter guidelines on the prescription, use and distribution of antibiotics .

The growing problem of antibiotic resistance has mainly stemmed from three different factors; patients failing to complete their antibiotic course, doctors over-prescribing antibiotics and bacterial adaptability leading to resistant strains like MRSA (methicillin-resistant Staphylococcus aureus).
To the first point, patients are prescribed antibiotics for a set duration depending on the specific antibiotic being administered at the time. Normally, being given a set duration to take antibiotics is given with the intent to completely eradicate the bacteria that exists in the system of the patient- failure to complete this can lead to some bacteria surviving and producing a new generation of the bacterial strain that forms immunity to the antibiotic because of genetic variability that exists in the bacterial culture.
So why do patients fail to complete their course? This normally is a result from patients feeling better before their course ends, because whilst most of the bacteria that were present have been eradicated as a result of the antibiotic, some may remain because they might have natural resistance to antibiotics as a result of the variability of the alleles that exist in the bacterial population.
To the second point, doctors contribute to antibiotic resistance through prescribing antibiotics. These are often considered 'broad-spectrum' because they can deal with a wide array of bacteria. This is beneficial for doctors, as they can often deal with bacterial infections quickly because of the probability that the broad-spectrum bacteria will be effective for the patient.
However this particular aspect also contributes to antibiotic resistance, as the constant broad spectrum antibiotics use which regularly targets protein productions in bacteria can lead to bacterial resistance, as species in a population that can prevent alterations to its protein production have become immune to many of the measures doctors use as a first resort to treating patients.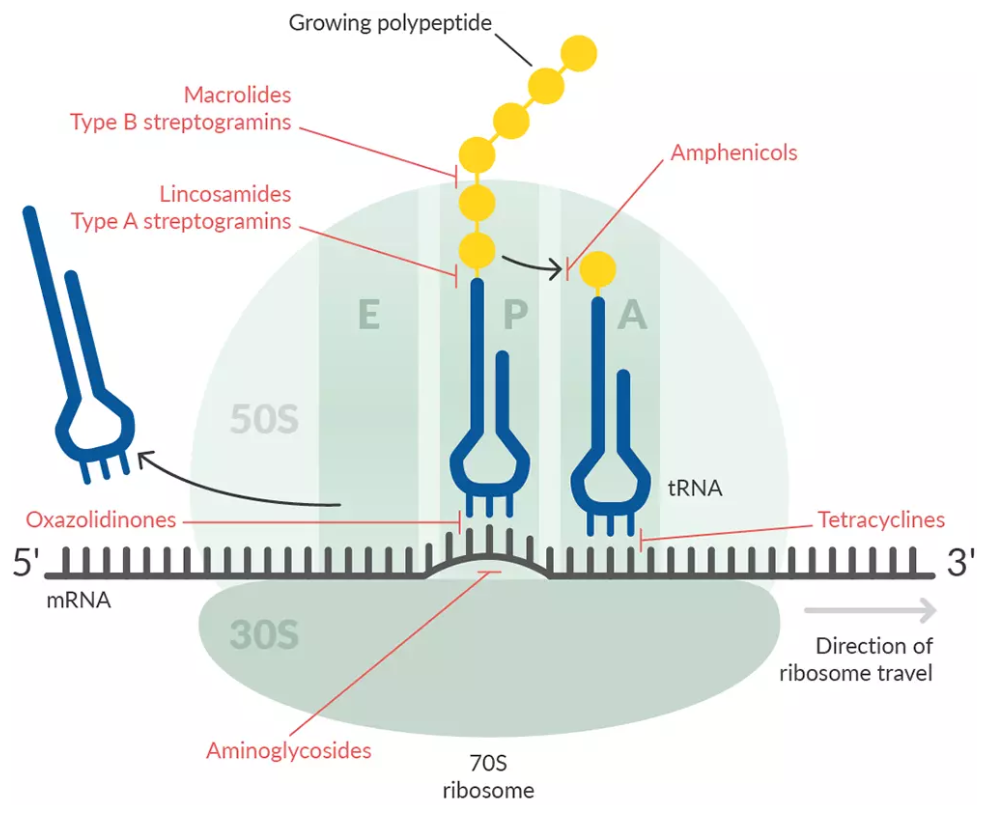
A good example of such a strain that has developed resistance in the hospital environment is the aforesaid MRSA strain, which has formed its resistance towards methicillin, which is one of the antibiotics used by doctors that take the broad-spectrum approach; methicillin targets the binding proteins which prevents peptide cross links from forming on the peptidoglycan which compromises the structural integrity of the bacterial cell-wall, which ultimately leads to the death of the bacteria.
However repeated use of this antibiotic in an environment that has a higher concentration of both the bacteria strain and the antibiotic which resulted in an increased probability of bacteria (which has natural resistance having an advantage over the other alleles) and hence through directional selection the allele for resistance against methicillin became advantageous and slowly MRSA developed its resistance. This is credited to the environment that the bacteria strain was in as it was constantly exposed to the mechanism that the antibiotic relied on hence it had the opportunity to combat this and prevent its own inhibition on the bacteria's activity.
 |
MRSA False colour(SEM)
|
When presented with the issue of antibiotic resistance the ever-present issue it creates and the future consequences that exist are clear. However, tackling the issue is not as clear cut, regardless there are some options that are proving effective against resistant bacteria.
One potential solution is restricting the use of broad spectrum bacteria and using specific treatment for bacteria based on the patient.
For example using antibiotics that are specific for Gram Positive (thick layers of peptidoglycan making its cell wall ) or Gram Negative (thin layer of peptidoglycan and a secondary lipopolysaccharide cell wall) . Narrow spectrum antibiotics are good because the chances that the bacteria will have resistance is reduced because the bacteria will not have readily encountered it so this reduces the chances of resistance.
Another benefit of specific antibiotics is that only the target bacteria will be removed. This is beneficial because it helps reduce adverse affects which broad spectrum antibiotics would have, as all bacteria would be affected. For example, gastrointestinal problems which can lead to other infections because the helpful bacteria that regulate the gut will be removed under the use of broad spectrum antibiotics .3
However this means that more time will be spent diagnosing patients and prescribing the appropriate antibiotic which might be time consuming for medical practitioners who have numerous patients to consult in a day.
Another approach that can be taken is to avoid resistance developing in the first place by regulating the distribution of antibiotics and creating awareness of the importance of completing a course of antibiotics . Communication that be made between a patient and the respective doctor and the emphasis of completing the course, regardless of symptoms improving. Regulation of antibiotics is also important as patients taking antibiotics thinking the cause of their symptoms is bacterial when in fact its viral is another opportunity for bacteria forming resistance to the antibiotic. Perhaps antibiotics should only be distributed with a physician's approval.
When presented with the issue of antibiotic resistance the ever present issue it creates and the future consequences that exist are clear however tackling the issue is not as clear cut, regardless there are some options that are proving effective against resistant bacteria.
One potential solution is restricting the use of broad spectrum bacteria and using specific treatment for bacteria based on the patient.
For example using antibiotics that are specific for Gram Positive (thick layers of peptidoglycan making its cell wall ) or Gram Negative (thin layer of peptidoglycan and a secondary lipopolysaccharide cell wall) . Narrow spectrum antibiotics are good because the chances that the bacteria will have resistance is reduced because the bacteria will not have readily encountered it so this reduces the chances of resistance.
Another benefit of specific antibiotics is that only the target bacteria will be removed. This is beneficial because it helps reduce adverse affects which broad spectrum antibiotics would have, as all bacteria would be affected (e.g. specific gastrointestinal problems).
The problem resistance causes is a complex one as a quick reliable method is needed for dealing with bacterial infections but balancing that with the need to preserve the methods that are being used today. Even distinguishing between bacterial and viral infections is often difficult as many elements are similar for both when it comes to symptoms. Regardless of the solutions implemented, action needs to be taken in order to prevent many reliable methods that are used by doctors today , decreasing in effectiveness which will result in the arsenal of doctors dwindling down slowly unless action is taken.
References:
Gottfried, J. (2005). History Repeating? Avoiding a Return to the Pre-Antibiotic Age. [online] dash.harvard.edu. Available at: https://dash.harvard.edu/bitstream/handle/1/8889467/Gottfried05.html.
FIDSA, J.R., MD (2017). Is the ‘full course of antibiotics’ full of baloney? [online] Harvard Health Blog. Available at: https://www.health.harvard.edu/blog/is-the-full-course-of-antibiotics-full-of-baloney-2017081712253
Dancer, S.J. (2020). The dangers of broad spectrum antibiotics. www.bmj.com. [online] Available at: https://www.bmj.com/rapid-response/2011/10/29/dangers-broad-spectrum-antibiotics.
Comments
Post a Comment